Contributing physicians in this story

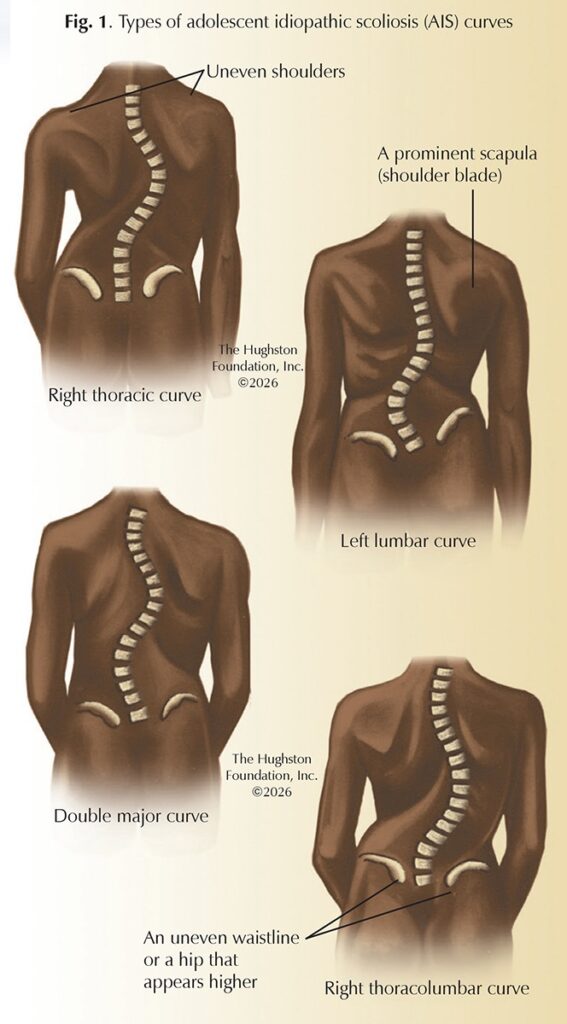
Adolescent idiopathic scoliosis (AIS), the most common type of spinal deformity that affects children, is characterized by an abnormal 3-dimensional curvature of the spine measuring 10 degrees or more (Fig. 1). The word “scoliosis” comes from the Greek term “skoliosis,” which means crookedness. Scoliosis is a deformity that causes the spine to curve to the side and the vertebrae to rotate into an abnormal position. The term “adolescent” signifies the onset between the ages of 10 and 18 years old, coinciding with the growth spurt of teenagers that begins at puberty. “Idiopathic” means that the cause of this spinal deformity is unknown, which distinguishes it from other, rarer types of scoliosis that result from congenital (present at birth) or neuromuscular (control of muscles by nerves) causes.
AIS is not rare, with an estimated prevalence of 3 to 5 percent of teenagers affected. In the United States, this translates to an estimated 6 to 9 million people living with scoliosis. The female-to-male ratio increases substantially with increasing size of curve, rising from 1.5 girls for every 1 boy in curves from 10 to 20 degrees, up to 10 girls for every 1 boy in curves greater than 30 degrees. While the prevalence of AIS affects millions of people, physicians manage most cases using bracing or other conservative treatments.
Clinical presentation and symptoms
AIS, a silent condition in its early stages, typically produces no pain or other symptoms; however, specific curve types, such as thoracic, lumbar, or thoracolumbar, can be physically noticeable. Often, it is first noticed by a parent, teacher, or during a routine school screening or physical examination. While mild back pain can occur, severe pain is not characteristic of AIS. Children with back pain should see their pediatrician for further evaluation.
Diagnosis
Early detection and treatment are crucial for managing scoliosis effectively, as curves are often easier to treat when they are smaller. An orthopaedist can diagnose AIS without any invasive or painful testing, using a combination of physical examination and x-rays.
The physical examination includes the Adam’s Forward Bend Test, which continues to be the cornerstone of clinical screening for the disorder (Fig. 2). The patient bends forward at the waist with their feet together, arms hanging down, and knees straight. From this position, the examiner can easily observe any asymmetry in the rib cage or lumbar region, known as a rib hump, which indicates rotational deformity of the spine.

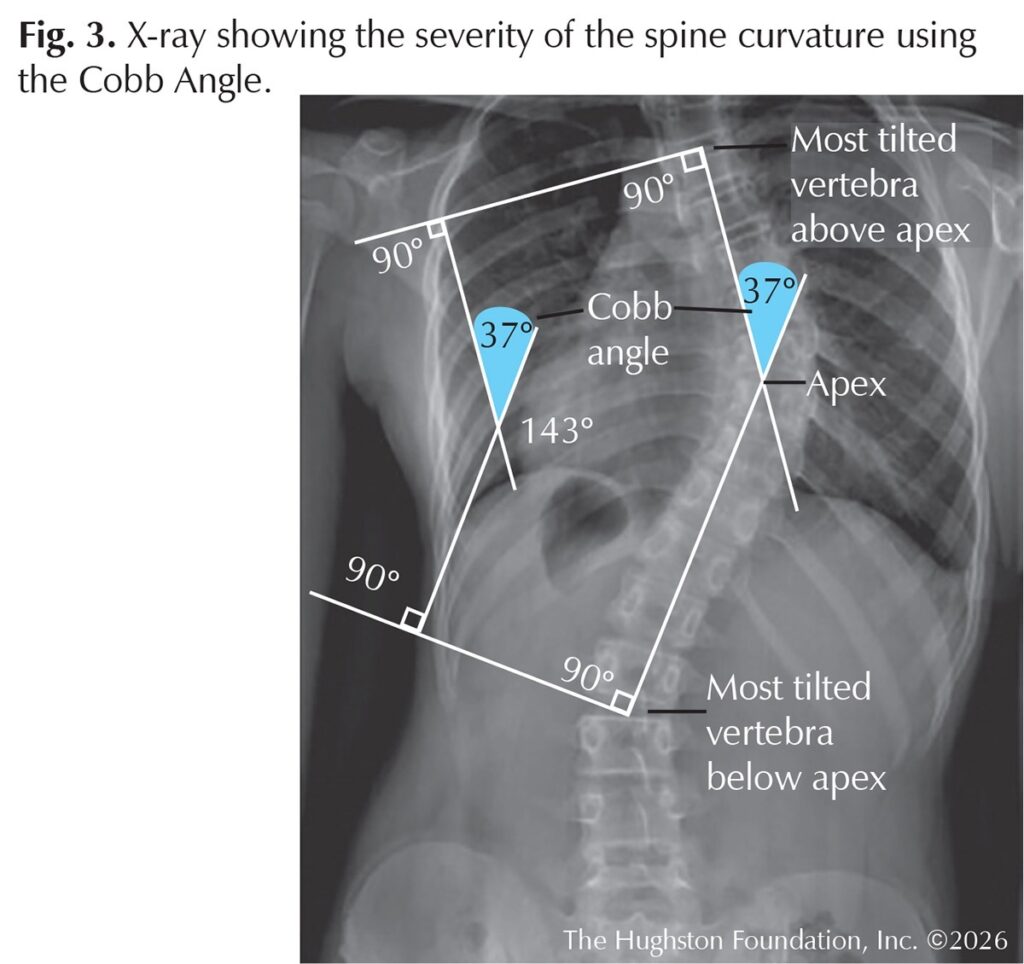
If the physician suspects scoliosis, standing x-rays of the entire spine, including frontal and side views, are ordered (Fig. 3). These images are important for visualizing the spinal curvature and confirming the diagnosis. The severity of the curvature can be measured using the Cobb angle, which is the standard method for quantifying the magnitude of the deformity. X-rays also aid with assessing the skeletal maturity of the adolescent to see whether the child is still growing, which helps predict the risk of progression. The x-ray also visually shows the physician the curve pattern, location, and direction of the curve.
Risk factors
Despite extensive research over the past 100 years, the exact cause of AIS remains elusive. Researchers have pointed to theories, such as genetics, hormones, biomechanical, and neuromuscular issues that may contribute to the condition. Although considered a multifactorial condition with several contributing elements, researchers have found that poor posture, carrying heavy backpacks, sports injuries, trauma, or diet do not cause the disorder.
AIS often runs in families, suggesting a strong genetic link. Research has identified several candidate genes, but scientists have not found a single causative gene. This leaves us with an inheritance pattern that remains complex and not fully understood. The condition’s emergence during the rapid growth of adolescence suggests that hormones and growth-related factors play a crucial role; however, their definitive role is unconfirmed. Some theories propose subtle abnormalities in the central nervous system, postural control, or the biomechanical properties of the spinal discs and ligaments (tissues that connect bones), which may lead to spinal instability and progressive curvature during growth. Unfortunately, even after extensive research, we do not have a proven theory explaining the cause of AIS.
Risk factors for curve progression
Sex: Females are diagnosed more often and have a higher risk of curve progression.
Curve magnitude: The larger the curve at the time of diagnosis, the more likely it is to worsen.
Skeletal immaturity: A growing individual has a longer window for the curve to progress.
Curve pattern: Certain curve patterns, such as double curves, may have a higher risk of progression than single curves.
Management and treatment
The primary goals of AIS treatment are to stop curve progression and prevent severe deformity; thereby, avoiding future health problems like chronic pain, or in very rare and severe cases, compromised lung function. Physicians base treatment decisions on the size of the spinal curve, whether the child is still growing, and observation of curve progression. The 3 main treatment strategies are observation, bracing, and surgery. Physicians treat approximately 90% of cases without the need for surgery.
- Observation: Many small curves do not progress and require no further intervention. For mild curves (a Cobb angle less than 20 to 25 degrees), the physician monitors the patient using regular clinical examinations and x-rays every 4 to 6 months to track any changes in the curve.
- Bracing: For moderate curves, typically 25 to 45 degrees, the physician may prescribe a brace while the patient continues to grow. Bracing does not correct the curve; it helps to prevent the deformity from progressing during the remaining growth period. For bracing to be effective, the patient should wear the brace for the prescribed number of hours per day, which can be from 16 to 23 hours per day.
- Spinal fusion surgery: Less than 10 percent of AIS cases require surgery. Physicians often recommend surgery for severe curves, greater than 45 to 50 degrees, or for curves that continue to progress despite bracing. Surgery can permanently correct a significant portion of the deformity and prevent any future progression.
Prognosis
For most adolescents, the prognosis for AIS can be excellent. With early detection and appropriate management, the vast majority of patients can lead full, active, and healthy lives with no physical limitations. Observation prevents unnecessary treatment for mild curves, while bracing can be an effective tool for halting the progression of moderate curves. For those with severe curves, modern surgical techniques offer reliable and lasting correction. Public awareness and screening programs remain vital for identifying at-risk individuals and ensuring they receive timely and effective care.
Authors: Joseph A. Martino, MD, FAAOS, and David P. Antekeier, MD, FAAOS | Atlanta, Georgia, and Columbus, Georgia
Last edited on April 10, 2026