
What is Tennis Elbow?
Lateral epicondylitis is a common painful condition of the elbow caused by overuse of the muscles of the forearm. Popularly known as tennis elbow because of its association with the sport, it is both a repetitive strain injury and a tendinopathy (diseased or abnormal condition of the tendon). Various studies have identified the repetitive wrist extension or forearm rotation and supination (turning toward the outside) involved in such activities as racquet sports and using heavy tools for manual labor as the primary risk factors for lateral epicondylitis. However, in many cases, the condition cannot be linked to any kind of precipitating activity and so is said to be of insidious onset (coming on slowly without obvious symptoms).
Regardless of the cause, once the muscles and the tendons (tissue that connects muscle to bone) that attach to the lateral epicondyle become chronically irritated and the attachment begins to degenerate, everyday activities, such as gripping or holding household objects, can be painful. Lateral epicondylitis affects 1 to 3% of the adult population, most often those between the ages of 30 and 50, and affects women slightly more often than men.
Elbow anatomy
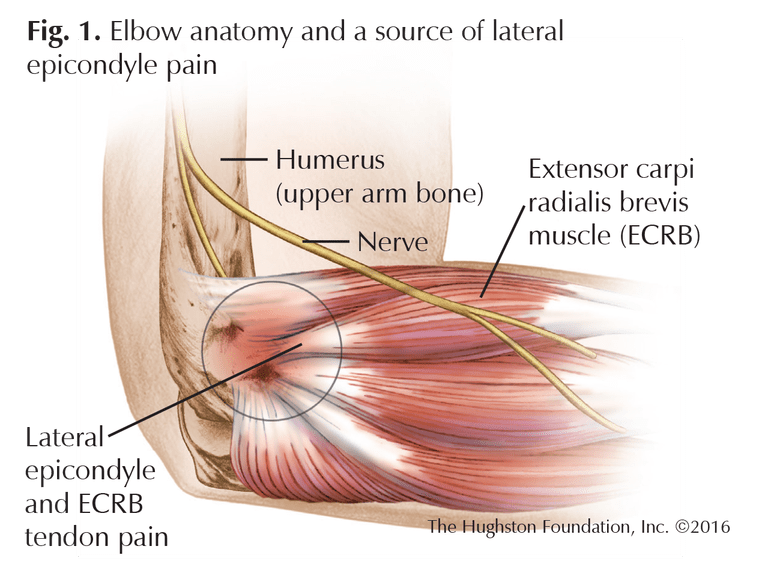
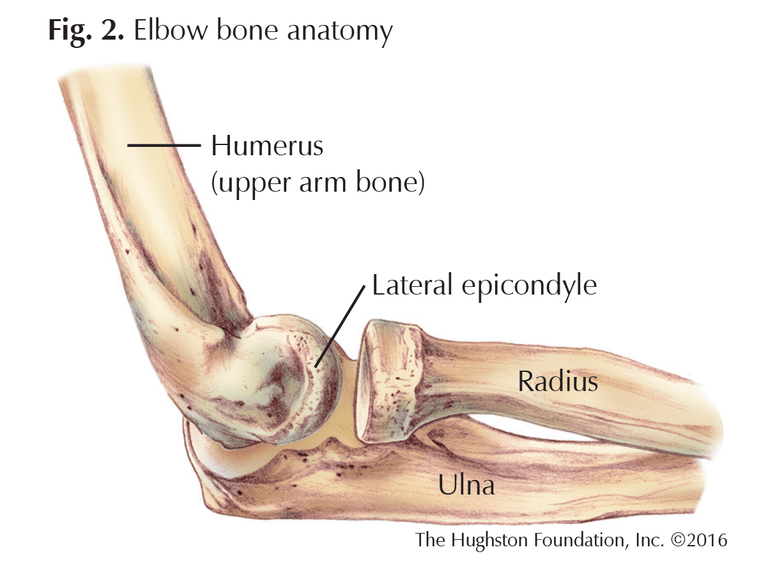
The elbow joint is held together by muscles, tendons, and ligaments (tissue that connects bones) (Fig. 1). It is a hinge joint that allows us to flex (bend), extend (straighten), and rotate the forearm. The bony projection that can be palpated on the outside of the elbow is the lateral epicondyle. It extends off the condyle, or rounded, knuckle-like bone ending, of the humerus (upper arm bone) which articulates with the radius and ulna (forearm bones) to form the joint (Fig. 2). The muscles that extend the wrist, such as the extensor carpi radialis brevis (ECRB), originate from the lateral epicondyle.
Sources of pain
The most common source of the pain associated with lateral epicondylitis is the ECRB muscle. Repetitive or overuse activities can cause microtrauma to the fibers of the muscle, resulting in microscopic tears and the release of inflammatory chemicals that induce pain. The pain may be a cause of the tendons that attach to the epicondyle or, alternatively, from conditions inside the joint, such as synovitis (inflammation of the synovium or joint lining) or plica band (inflammation and enlargement of a part of the joint lining). Typically, the pain is felt on the outside of the elbow in the portion of the ECRB closest to the joint, and the lateral epicondyle itself may be tender. The pain of lateral epicondylitis can be reproduced with resisted wrist and finger extension, and most patients complain of a weak and painful grip.
Nonsurgical treatment options for Tennis Elbow
The majority of lateral epicondylitis or tennis elbow cases resolve on their own without formal treatment. When pain persists, it usually prompts a person to visit a physician or orthopedist. The appointment will include a detailed history, physical exam, and x-rays; if the problem is severe enough, the doctor may order an MRI.
Standard nonoperative treatment for lateral epicondylitis consists of taking oral nonsteroidal anti-inflammatory drugs (NSAIDs), modifying activity, using orthotic braces (such as tennis elbow straps), and undergoing physical therapy. Another nonsurgical measure is to inject steroidal medication directly into the identified site to decrease pain and inflammation. With the effectiveness of steroid injections in question, some novel injection techniques are emerging. For example, an autologous (from one’s own body) platelet concentrate (consisting mainly of blood plasma and platelets or cell fragments involved in clotting) can be injected into the affected elbow to stimulate a healing response. Also known as platelet-rich plasma (PRP) therapy, these injections have shown promising results in some studies, but more research is needed to determine their real efficacy.1,2 It is also important to note that between 80 and 95% of all cases of epicondylitis resolve without operative treatment.
Surgical treatment options for Tennis Elbow
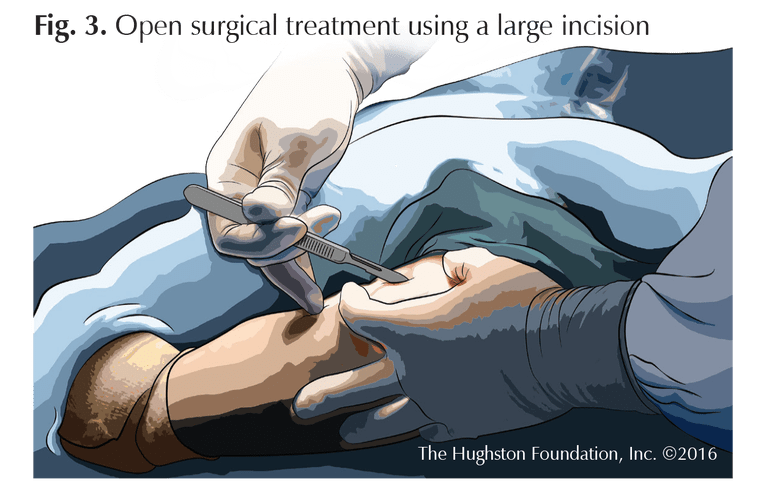
When refractory or stubborn cases of lateral epicondylitis fail to respond to nonoperative treatment, surgical options can be considered. Traditional surgery for tennis elbow has consisted of large, open techniques that expose the extensor muscles and identify and excise (remove) the damaged tissue (Fig. 3). Such procedures typically include tendon repair by reattaching healthy tissue to the bone. More recently, less invasive surgical techniques, such as arthroscopy (inserting a tiny fiber-optic video camera and instruments into the joint) have been developed. Unlike traditional open surgery, arthroscopic treatment of lateral epicondylitis requires only a small percutaneous (through the skin) incision and a shorter recovery period. It also allows the surgeon to identify and treat any additional intra-articular pathology (disease process within the joint).
New treatment
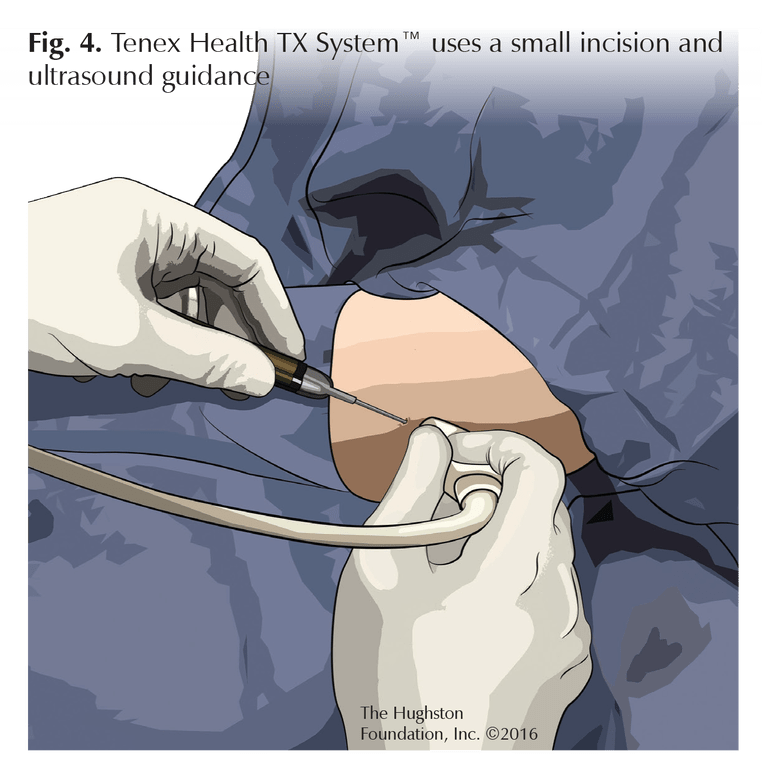
A new minimally invasive technique known as a percutaneous tenotomy (tendon resection) that uses the Tenex Health TX System™ is currently evolving. The procedure uses a percutaneous incision and ultrasound guidance above the skin rather than a scope to identify diseased tissue (Fig. 4). A special hand-held tool is then used to mechanically break up the tissue and flush it out.3
Preliminary research on this treatment has been promising. One recent study including a 3-year follow-up showed excellent functional outcomes and high patient satisfaction.4
Additionally, postprocedure ultrasound evaluation of the tendon showed a good tissue-healing response in the diseased area. The theoretical advantages of this technique over other techniques include:
- a much smaller incision
- the ability to target the diseased area with minimal disruption to healthy tissue
- decreased postoperative pain
- a shorter recovery period.
Despite these advantages, we need more research to establish this procedure as a preferred treatment for lateral epicondylitis.
Good results
Lateral epicondylitis or tennis elbow is a common yet potentially debilitating condition that can limit the performance of everyday activities. While most cases resolve on their own or with nonsurgical treatment, more difficult or refractory cases may require surgery. When surgery is necessary, new arthroscopic and other minimally invasive techniques, particularly percutaneous tenotomy with Tenex Health TX System™, have shown good results for patients.
Author: David A. Lalli, DO | Columbus, Georgia
References:
1. Peerbooms JC, Sluimer J, et al. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. American Journal of Sports Medicine. 2010;38(2):255-62.
2. Gosens T, et al. Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis: a double-blind randomized controlled trial with 2-year follow-up. American Journal of Sports Medicine. 2011;39(6):1200-08.
3. Barnes DE, Beckley JM, Smith J. Percutaneous ultrasonic tenotomy for chronic elbow tendinosis: a prospective study. Journal of Shoulder and Elbow Surgery. 2015;24(1):67-73.
4. Seng C, Mohan PC, Koh SB, et al. Ultrasonic percutaneous tenotomy for recalcitrant lateral elbow tendinopathy: sustainability and sonographic progression at 3 years. American Journal of Sports Medicine. 2016;44(2):504-10.
Reprinted with permission from the Hughston Health Alert, Volume 28, Number 3, Summer 2016.
Last edited on August 2, 2026